Nonmelanoma Skin Cancer: Basal vs. Squamous Cell Carcinoma - Key Differences and What You Need to Know
 Jan, 26 2026
Jan, 26 2026
Most people think of melanoma when they hear "skin cancer." But the truth is, basal cell carcinoma and squamous cell carcinoma are far more common-and they’re both types of nonmelanoma skin cancer. Together, they make up about 95% of all nonmelanoma cases. You might not have heard much about them, but if you’ve spent time in the sun, especially over many years, you’re at risk. The good news? Both are highly treatable when caught early. The catch? They’re not the same. Knowing the difference could save your life.
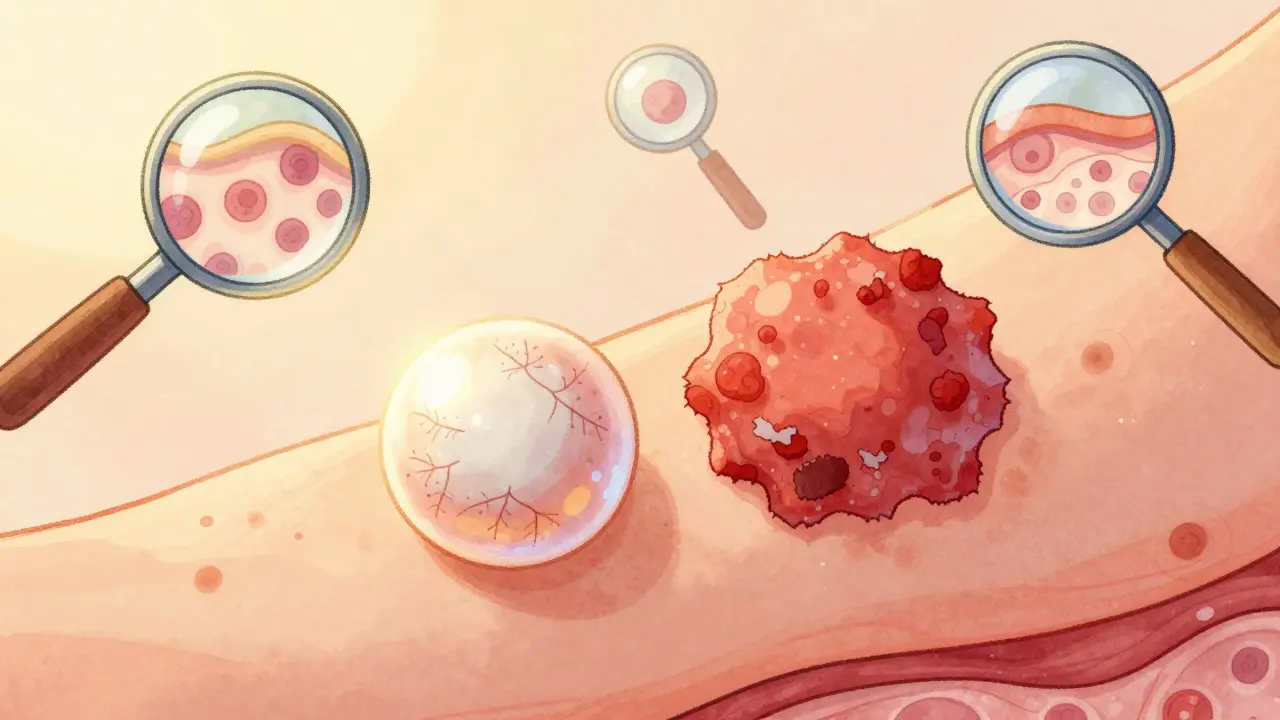
Where They Start: The Skin’s Layers
Your skin has layers. The top layer, called the epidermis, is made up of flat, scale-like cells called squamous cells. Below them, in the deepest part of the epidermis, are round basal cells. These basal cells constantly divide, pushing older cells upward. As they rise, they flatten out and become squamous cells. That’s why basal cell carcinoma starts deep, and squamous cell carcinoma starts on top.Basal cell carcinoma (BCC) forms from those deep basal cells. It grows slowly, often taking years to become noticeable. Squamous cell carcinoma (SCC) starts in the upper layer, where cells are already flat and exposed. Because it’s closer to the surface, it can grow faster and spread more easily.
What They Look Like: Spotting the Signs
You don’t need a doctor to notice something’s off. Here’s what to watch for:Basal cell carcinoma usually shows up as:
- A shiny, pearly bump-often with tiny blood vessels visible on the surface
- An open sore that bleeds, oozes, or crusts and never fully heals
- A scar-like patch that’s flat, white, or yellow, and feels firm to the touch
Squamous cell carcinoma tends to look like:
- A firm, red bump that grows quickly
- A flat, scaly, reddish patch that might crust or bleed
- A wart-like growth that feels rough
- An open sore that won’t go away, even after weeks
Both can be mistaken for a pimple, eczema, or a scar. But if something doesn’t heal after four to six weeks, especially on your face, ears, neck, or hands, get it checked. Don’t wait.
How Fast They Grow: Speed Matters
BCC creeps along. On average, it grows about half a centimeter to one centimeter per year. That’s why many people ignore it for months-or even years. It doesn’t hurt. It doesn’t itch. It just sits there, slowly eating away at your skin.SCC doesn’t wait. It can grow 1.5 to 2 centimeters in a year-and some aggressive forms double in size in just four to six weeks. People often notice SCC because it changes fast. A spot that was barely there last month is now raised, bleeding, or painful. That’s a red flag.

How Dangerous They Are: Metastasis Risk
Here’s where the big difference lies. BCC almost never spreads. Fewer than 0.1% of cases become metastatic. Even if left untreated for years, it usually just destroys tissue locally-eating through skin, cartilage, or bone on your nose, ear, or eyelid.SCC is different. While most cases are still caught early and cured, about 2% to 5% of SCCs spread to lymph nodes or other organs. That number jumps to 14% if it’s on your lip, 9% if it’s on your ear, and 7% if it’s on your genitals. Once it spreads, survival rates drop from 95% to 25-45%. That’s why doctors treat SCC more aggressively from the start.
Who Gets It: Risk Factors
Both cancers are linked to sun exposure. But the pattern matters.BCC often shows up in people who’ve had intense, occasional sunburns-think weekend beach trips or childhood sunburns that blistered. It’s common in fair-skinned people over 50, and slightly more common in men (55% of cases).
SCC is tied to long-term, cumulative sun exposure. Think farmers, construction workers, or anyone who’s spent decades outdoors. It’s also more common in men (65% of cases), likely because of occupational exposure. People with weakened immune systems-like organ transplant recipients-are 250 times more likely to develop SCC than BCC.
Age plays a role too. The average age for BCC diagnosis is 67. For SCC, it’s 69. But both are rising in younger adults, especially in places like Australia and the UK, where UV levels are high.
Treatment: What to Expect
Both cancers are treated with surgery, but the approach differs.For small, low-risk BCC, doctors often use:
- Topical creams like imiquimod or 5-fluorouracil (effective in 60-70% of cases)
- Curettage and electrodessication (scraping and burning)
- Standard surgical removal
For SCC, especially if it’s larger than 2 cm, deeper than 2 mm, or on the ear/lip, doctors go straight to:
- Mohs surgery (the gold standard-97% cure rate for SCC)
- Wider surgical margins (4-10 mm vs. 3-5 mm for BCC)
- Radiation or immunotherapy if it’s spread
Immunotherapy drugs like cemiplimab (Libtayo) are now approved for advanced SCC that can’t be surgically removed. There’s no equivalent drug for BCC yet-though hedgehog inhibitors like vismodegib work well for advanced cases.
On average, SCC patients need 1.8 treatment sessions. BCC patients need just 1.2. Why? SCC often needs more tissue removed to make sure it’s all gone.
Recovery and Follow-Up
Most people recover fully after treatment. But follow-up matters.BCC patients usually need check-ups every 12 to 18 months. SCC patients? Every 6 to 12 months. Why? SCC is more likely to come back-and it’s more likely to come back fast. About 73% of recurrent SCC cases show up within a year. For BCC, it’s closer to 18 months.
Patients with SCC also report higher anxiety. In patient surveys, 85% of SCC patients worried about metastasis. Only 42% of BCC patients did. That’s not just fear-it’s reality. SCC has a higher chance of spreading. And once it does, treatment becomes harder, costlier, and less effective.
Prevention: What Actually Works
The best treatment is no treatment at all. Prevention works.Daily sunscreen reduces BCC risk by 40%. For SCC, it cuts risk by 50%. Why? Because SCC is more tied to long-term UV exposure, not just sunburns. So wearing sunscreen every day-even in winter, even if it’s cloudy-isn’t optional. It’s essential.
Wear a wide-brimmed hat. Seek shade between 10 a.m. and 4 p.m. Avoid tanning beds completely. They increase your risk of both cancers by up to 60%.
If you’ve had one skin cancer, your risk of another skyrockets. That’s why people with a history of BCC or SCC are advised to see a dermatologist every 6 to 12 months. Don’t skip these visits.
The Bottom Line
Basal cell carcinoma is the most common cancer in humans. But squamous cell carcinoma is the one you need to take more seriously. It’s less common, but more dangerous. It grows faster. It spreads more often. It demands quicker, more aggressive action.Neither is a death sentence. Both are highly curable-when caught early. The key is knowing the signs, checking your skin monthly, and seeing a doctor the moment something doesn’t heal. Your skin is your largest organ. Protect it like you protect your eyes or your heart.
And if you’ve ever had a sunburn that blistered, or spent years working outside without protection? You’re not too old to start being careful. It’s never too late.
Candice Hartley
January 27, 2026 AT 10:52Just checked my arm and found a weird pearly bump I thought was a zit... 😳 Thanks for the clarity. Going to the derm tomorrow. No more ignoring stuff!
astrid cook
January 28, 2026 AT 20:34Ugh. Another one of those "sun exposure is bad" lectures. Like anyone actually cares anymore. We're all gonna die anyway. 🙄
Kegan Powell
January 28, 2026 AT 23:52Man I've spent half my life working construction under the sun and never thought twice about it... now I'm realizing how lucky I've been. This post hit different. Thanks for laying it out so plainly. We don't talk enough about how silent these cancers can be. Just be kind to your skin, folks. It's been carrying you since day one 🙏
suhail ahmed
January 29, 2026 AT 12:34Love how this breaks it down like a chai latte - smooth, layered, and gives you warmth after the sip. BCC is like that slow drip of rain on your roof - you don’t hear it until the ceiling caves. SCC? That’s the thunderclap that wakes you up screaming. And yeah, sunscreen isn’t optional, it’s your skin’s kryptonite shield. Also, hats > hats off. Wear the damn thing.
Anjula Jyala
January 29, 2026 AT 16:59Actually the metastasis stats are misleading because they don't adjust for anatomical location bias and sampling error in dermatology databases. Also the 50% risk reduction from sunscreen is from observational studies with confounding variables. You should really cite the Cochrane review. Also, most people don't apply enough sunscreen anyway so the numbers are inflated. Stop fearmongering.
Kirstin Santiago
January 31, 2026 AT 04:46I’m 42 and got my first BCC last year. It was on my nose. They scraped it off in 10 minutes. No big deal. But now I wear SPF 50 every single day. Even indoors. Even when it’s raining. My dermatologist says I’m lucky it was caught early. Honestly? I’m just glad I didn’t ignore it like I used to ignore everything.
Kathy McDaniel
January 31, 2026 AT 09:44i just checked my hand and theres this one spot that been there for like 3 months?? i thought it was dry skin but now im scared lol. going to the doc next week. thanks for the nudge 😅
April Williams
February 1, 2026 AT 16:19Why are we still letting people live like this? No one wears hats anymore. No one checks their skin. You think sunscreen is enough? You think a quick swipe is protection? You’re not protecting yourself-you’re deluding yourself. And then you wonder why cancer is rising. It’s not bad luck. It’s negligence. And you’re all complicit.
Harry Henderson
February 2, 2026 AT 23:17STOP WAITING. If it’s been there longer than two weeks and it’s not a pimple-GET IT CHECKED. I had SCC on my ear. Thought it was a bug bite. Took 8 months to diagnose. Now I have a scar the size of a quarter and a whole new respect for dermatologists. Don’t be me. Act now. Your future self will thank you.
Andrew Clausen
February 3, 2026 AT 07:55The article misstates the cure rate for Mohs surgery. It's 97% for primary SCC, not all SCC. Recurrent cases drop to 94%. Also, hedgehog inhibitors are not exclusive to BCC-sonidegib is also used off-label for SCC in some cases. And sunscreen reduces risk, but the 40-50% figures are meta-analytic averages with wide confidence intervals. Precision matters.
John O'Brien
February 4, 2026 AT 16:36Man I used to think skin cancer was just for old folks or beach bums. Then my dad got SCC on his lip after 40 years of farming. He didn’t even know it was cancer till it started bleeding. Now he wears a hat 24/7 and makes me put on sunscreen before I even leave the house. Honestly? Best thing he ever did. Don’t wait till it’s your turn.